Mitigating Risk in Healthcare: Learning from Bad Outcomes
Mitigating Risk in Healthcare: Learning from Bad Outcomes
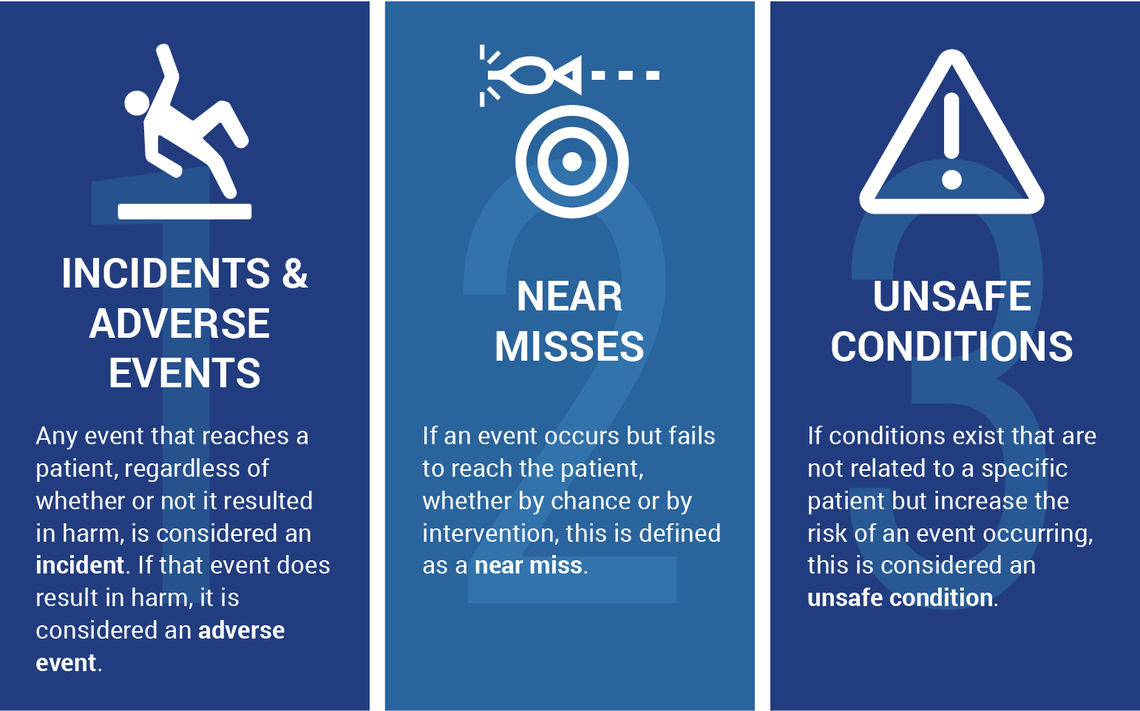
Adverse events include a variety of unintended outcomes that cause patient’s harm. “Every year, millions of Medicare patients experience adverse events and temporary harm events as a result of medical care or in a health care setting.” (OIG, 2023). In such cases, patients may incur prolonged hospitalization/treatment and permanent harm. Patient death is also associated with adverse outcomes. When patient safety is compromised, it is up to the organization to conduct a comprehensive investigation to determine how the event occurred. If concerns are not addressed, the probability of the event reoccurring is highly likely.

Risk Mitigation Strategies
Although hospitals strive to ensure they have a comprehensive Quality Assure Performance Improvement (QAPI) Program, there are several considerations to ensure that such programs are effective. To have a state-of-the-art electronic reporting program is simply not enough. It is important to ensure that that the following elements are in place:

- Establishing a culture of safety. Empowering employees to report concerns before they lead to adverse events.
- Educating healthcare personnel on how to report risks or concerns.
- Following up immediately on events that are reported.
- Conducting a root cause analysis or gap analysis to evaluate events preceding an adverse outcome. Findings should be communicated as appropriate to prevent recurrence.
- Performance Improvement (PI) measures should be considered using a multidisciplinary approach. Be sure to educate team members on new PI initiatives.
- Safety measures should be implemented without delay.
- Data collection and ongoing monitoring are critical to ensure that performance measures are effective. In the event that safety measures are not working well, revaluation is required, and new improvement strategies should be considered.
- Near-miss events should also be reported and monitored. Establishing or re-establishing standard operating procedures may be necessary to prevent patient harm.
“A coordinated team approach where everyone is on the same team and empowered to express their concerns irrespective of "rank," and members are knowledgeable about their duties, offers the best chance for successful risk mitigation” (McGowan, et al 2023). Establishing and setting the tone for safe culture in healthcare settings is a must. Ongoing training on quality initiatives and process improvement is necessary to promote safe culture. Employees who do not “buy in” may also have a negative impact on their peer’s willingness to report concerns. A leadership team that fosters accountability, teamwork and transparency will have a positive impact on employee engagement and satisfaction.
There is no time like the present to take a closer look at your organization’s risk mitigation strategies. Are you looking for expert guidance on QAPI Program enhancement or Risk Mitigation strategies? HCE Global offers specialized consulting services to help your facility navigate regulatory challenges and achieve operational excellence.
Our experts understand the challenges that all healthcare facilities are facing today. Using a customizable approach, we will help you navigate through even the toughest of challenges.
Whether you are in need of QAPI assistance, mock surveys, leadership training, corrective action plans or ongoing routine support services, we can help!
We pride ourselves on helping our clients achieve and maintain a status of excellence in the healthcare industry.
Be sure to browse Our Website for a full list of services we provide.
Contact us today at (800) 813-7117 to schedule a free consultation.
References:
McGowan J, Wojahn A, Nicolini JR. Risk Management Event Evaluation and Responsibilities. [Updated 2023 Aug 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559326, https://oig.hhs.gov/reports/featured/adverse-events