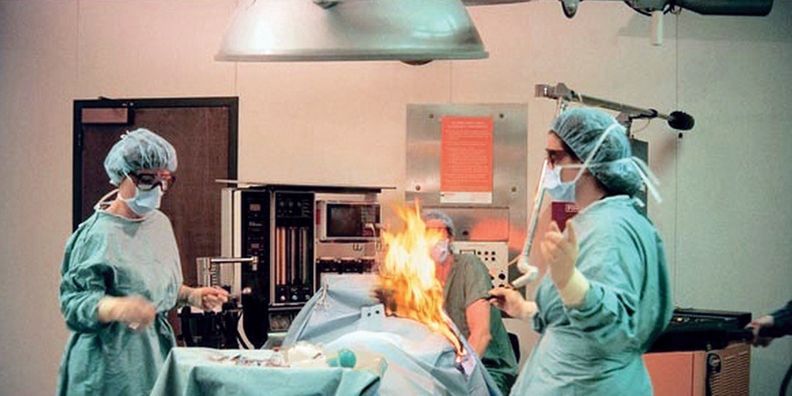
Fire on the Table
Confident Your Surgical Team is Prepared?
August 2023
By Jody Randall MSN, RN, CIC, HACP-CMS, HACP-PE
CEO and Founder
“Operating room fires are devastating events that occur at least 650 times annually.” (FDA, 2018). Healthcare facilities are required to perform fire drills routinely.
We find that often, the requirement of performing routine fire drill requirements sometimes overshadows the need to perform drills specific to surgical services. Although fires can occur anywhere and at anytime for a variety of reasons, what we do know is that there are three key elements that contribute to an increased risk of fire occurring in a surgical environment.
It is important to also consider that surgical fires can also occur during office-based procedures and therefore fire drills should also be conducted in these settings.
There are three key elements to contribute to the perfect environment for a fire to occur. Fuels, ignition sources and oxidizers are frequently used in combination in surgical procedures. You can see examples of each element below in what is known as the fire triangle:
{continues after in-line photo courtesy of Image Resource - Jones, et al.; 2017}

Fire Risk Assessment and "Time Out"
Performing a fire risk assessment as part of “time out” prior to performing a surgical procedure is also best practice. The Association of PeriOperative Registered Nurses (AORN) has created the following
Fire Risk Assessment tool
.
It is important to evaluate practices in your organization. Here are a few questions to determine if your organization is truly prepared for this type of disaster:
- Are team members including fire risk assessments as part of their time out procedure?
- Are dry times for skin preps being properly observed?
- Do team members understand the elements that contribute to surgical fires?
- Have they been educated on their role in the event of a fire?
- How to activate alarm and overhead announcement system?
- Who can shut of medical gases and where are the valves located?
- How to extinguish a fire?
- Where and how to evacuate the area safely?
- Do they know how to report an event that has occurred or a near miss?
The Joint Commission (TJC) Environment of Care Standard EC.02.03.01 EP11 requires organizations to:
Periodically evaluate potential fire hazards that could be encountered during operative or invasive procedures
Establish written fire prevention and response procedures, including safety precautions related to the use of flammable germicides or antiseptics
Risk factors should not be overlooked by any member of the surgical team. It is important to consider that patients are often sedated during procedures. Each member of the surgical team has a responsibility to protect the patient from harm. Patients may not be able to respond immediately to a burning sensation.
“Of 114 cases identified involving surgical fires, 60% of these resulted in a median award of $215000 to the plaintiff”. (Choudhry, et al., 2017). Adverse outcomes do not only lead to litigation, financial burdens and poor publicity but can also lead to increased anxiety, low morale, and increased turnover among personnel.
It is important for executive leadership to take a supportive approach regarding fire safety and emergency management planning. It is also important for team members to be able to report concerns that they may have about lack of adherence to safety protocols. Does your organization have a system in which team members can safety report concerns without fear or repercussions?
At HCE, we understand the nature of the healthcare environment can be stressful and fast-paced. Safety should always be a number one priority and never overlooked for the sake of taking shortcuts. We encourage all healthcare leaders to take a deep dive into their organizations’ current practices ensuring that safety continues to be a top priority.
HCE is Here to Help
Healthcare Consulting Experts LLC was built based upon our understanding of the challenges that healthcare facilities are facing today. Healthcare professionals strive to deliver the best possible care to all patients. We can help your facility through the difficult times and put you back on track to a less stressful tomorrow.
Don’t take chances! Our experts can assist with regulatory compliance requirements for whether you are building a new, state-of-the-art project or renovating an existing structure. Be sure to visit Our Website to see a full list of the services that we provide.
Contact us today at +1 (800) 813-7117 for a free initial consultation.
Please join us by clicking on any of our icons below to leave a comment or for more informati
on and updates.
References:
https://www.aorn.org/guidelines-resources/tool-kits/fire-safety/tool-kit
Choudhry AJ, Haddad NN, Khasawneh MA, Cullinane DC, Zielinski MD. Surgical Fires and Operative Burns: Lessons Learned From a 33-Year Review of Medical Litigation. Am J Surg. 2017 Mar;213(3):558-564
http://www.fda.gov/Drugs/DrugSafety/SafeUseInitiative/PreventingSurgicalFires/default.htm
Jones EL, Overbey DM, Chapman BC, Jones TS, Hilton SA, Moore JT, Robinson TN: Operating room fires and surgical skin preparation. J Am Coll Surg 2017; 225:160–5
https://pubs.asahq.org/anesthesiology/article/130/3/492/19230/Operating-Room-Fires